
Part 3 in our video series Performing the Mat Evaluation with blog content by Ana Endsjo, MOTR/L, CLT and video by Stacey Mullis, OTR/L, ATP. See Part 1 and Part 2.
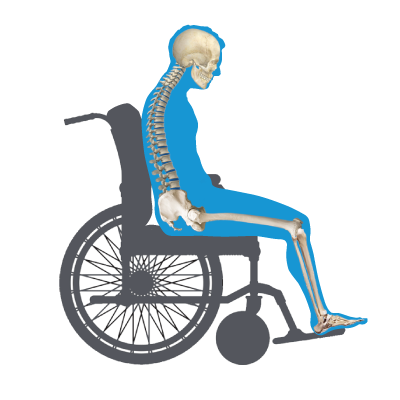
Probably the most commonly seen postural abnormality is a posterior pelvic tilt, frequently referred to as “sacral sitting.” This is the presentation of someone sliding down in the chair with very rounded shoulders. The anterior superior iliac spine (ASIS) is higher than the posterior superior iliac spine (PSIS), causing the client to sit directly on the sacrum and leaving it at high risk for a pressure injury.
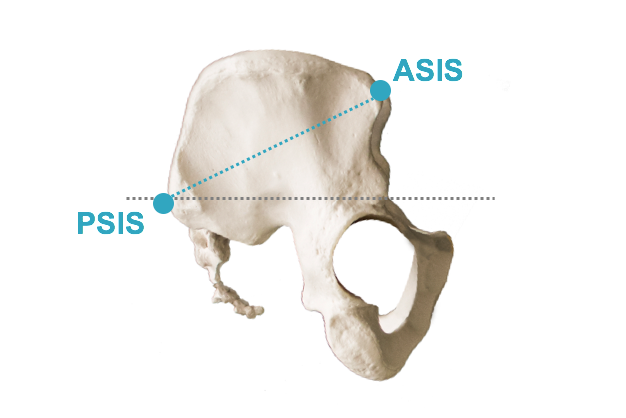
The easiest way to palpate for a posterior pelvic tilt is to locate the ASIS. You will notice that the PSIS will be difficult to find in this posture as they will be lower and almost “under” the client. Recall the little tricks we provided in the first blog of this series to make finding those bony landmarks a little easier:
- ASIS: known as the “hip bones.” These are the bones that stick out in the front of our pelvis and where we often rest our hands.
- PSIS: Look for the “dimples” or indentations in the lower back and then push deep into that area to palpate the PSISs.
With a posterior pelvic tilt, the trunk and head are affected as well.
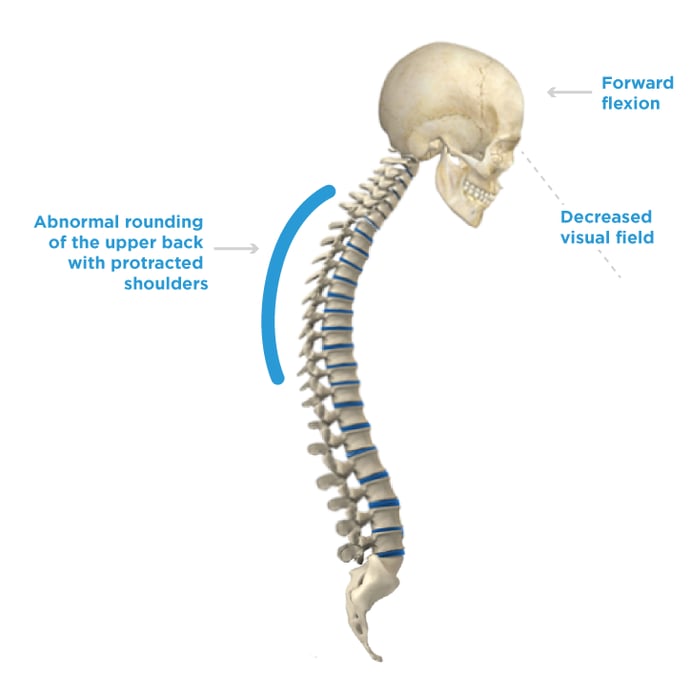
- The spine presenting with an excessive “C” curvature of the spine with the shoulders protracted (rounded shoulders).
- The head goes into a forward flexion, and the client has lost pretty much all visual field, looking straight down at their lap or the floor.
Let’s look at this week’s short video clip of the live mat evaluation presented by Stacey Mullis to increase confidence with the hands-on portion of the mat evaluation. Stay tuned for next week when we look at anterior pelvic tilt.
Transcript (edited for clarity):
Another common posture that you probably see all the time is a posterior pelvic tilt. Let’s take a look at how we would assess for that and determine if that is what is really going on.
Again we have to start with the pelvis; I’m going to reach in here and feel Jamie’s ASIS. The other landmark that you need to be aware of with this posture is the posterior superior iliac spine (PSIS). In order to palpate this, you’re going to have to get behind your resident. On your own you can feel the rear of your pelvis where those dimples are, and that’s going to be your PSIS. That’s what you’re looking for with your resident; just palpate for where those dimples are and then you’re going to feel the PSIS.
Now I don’t know if you can see but with the posterior pelvic tilt the PSIS is going to be lower than the ASIS which is right here. If I palpate her ASIS again, her PSIS is going to be lower. We can see clearly that she’s in a posterior pelvic tilt.
Another great indicator of posterior pelvic tilt is her overall posture; she has a kyphotic posture with her shoulders rolling forward and her head is pointing down. These are classic signs of a posterior pelvic tilt.

Ana Endsjo, MOTR/L, CLT
Clinical Education Manager LTC Division
Ana Endsjo has worked as an occupational therapist since 2001 in a variety of treatment settings. She has mainly worked with the geriatric population, dedicated to the betterment of the treatment of the elderly in LTC centers. Her focus has been on seating and positioning and contracture management of the nursing home resident. With this experience, her hope is to guide other therapists, rehab directors, nurses, and administrators through educational guides, blogs, webinars, and live courses in her role as Clinical Education Manager for the long term care division.