When it comes to assessing our clients’ posture and problem solving what can be achieved through the seating system, it is critical that we are familiar with the common postural abnormalities seen in wheelchair seating and positioning.
What am I looking at? What is the body doing that it shouldn't be doing?
Before we can assess for any abnormal postures that need to be corrected or accommodated in the wheelchair system, we must first understand neutral posture in order to assess any variance from “normal”.
Neutral Pelvic Position

What is the pelvis doing?
Pelvis in midline.
ASIS & PSIS at equal height: no pelvic tilt
L ASIS & R ASIS at equal height: no pelvic obliquity
L ASIS & R ASIS at equal depth: no pelvic rotation
What is the spine doing?
Spine is balanced and upright, no rotation, no lateral curvature. Normal lordosis in cervical and lumbar spine and normal kyphosis in thoracic spine creating the desired “S” shape.
What is the head doing?
Head is functionally upright with possible mild forward/lateral flexion or rotation.
ABNORMAL POSTURES
Next, we will begin to examine abnormal postures. Let’s take a look at the most common abnormal postures seen in wheelchair seating and positioning; they can be grouped into 5 categories:
Posterior Pelvic Tilt with thoracic kyphosis & forward neck flexion, a.k.a. “sacral sitting”:

What is the pelvis doing?
Pelvis sits with ASIS higher than the PSIS resulting in the posterior pelvic tilt, which produces the “sacral sitting” posture.
What is the spine doing?
Excessive thoracic kyphosis, producing “C” shape spine
“Flattening out” of the lordosis of the cervical spine
“Flattening out” of the lordosis of the lumbar spine
What is the head doing?
Decreased lordosis in cervical spine, causing forward neck flexion & downward eye gaze to floor/lap
*This can results in decreased interaction with the environment, difficulty with eating/swallowing, impaired respiration, and compromised ability to perform ADLs.
Anterior Pelvic Tilt with lumbar lordosis & neck hyperextension:

What is the pelvis doing?
Pelvis sits with PSIS higher than the ASIS, resulting in the anterior pelvic tilt.
What is the spine doing?
Excessive lordosis of the lumbar and cervical spine: the individual hyperextends his back over the sling back of the chair, placing him at risk of tipping the chair backwards.
What is the head doing?
Excessive lordosis of cervical spine causes hyperextension of the neck and upward eye gaze.
*This can result in decreased interaction with the environment, difficulty with eating/swallowing, impaired respiration, and compromised ability to perform ADLs.
Pelvic Rotation with rotation of the spine & lateral neck flexion:
What is the pelvis doing?
Pelvis sits with L or R ASIS more forward than the other, producing a rotation in the hips.
What is the spine doing?
The thoracic spine follows and rotates in the same direction as the pelvis. Therefore, if the right side of the pelvis is rotated more forward, the right side of the spine is rotated more forward as well.
What is the head doing?
The neck will go into lateral flexion as if the person is dropping the ear to his or her shoulder.
|
Tip: There are two ways of naming pelvic rotation; one for more forward ASIS/PSIS and the other for the direction the pelvis is rotated towards. So, be sure to be descriptive of the position of the pelvis in your documentation so that the payer understands clearly why you are requesting the specific equipment needed to address this issue! |
Pelvic Obliquity with scoliosis & lateral neck flexion:

What is the pelvis doing?
Pelvis sits with the L or R ASIS/IT higher than the other, causing the raising up of one hip relative to the other.
What is the spine doing?
When one side of the pelvis is raised higher than the other, the thoracic spine curves away from the higher side creating a scoliosis.
What is the head doing?
The neck will go into lateral flexion as if the person is dropping the ear to his or her shoulder. The lateral flexion will usually be towards the side where the hip is higher.
|
Tip: Pelvic obliquities are named for the side of the lower ASIS/IT. So, in the picture above, this would be called a RIGHT pelvic obliquity. |
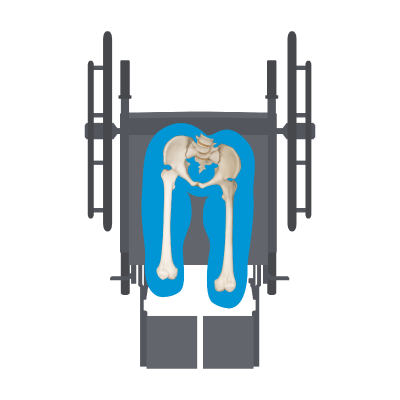
Windswept Deformity

What is the pelvis doing?
Usually goes hand in hand with a rotation and/or an obliquity and causes one leg to ADDuct/internally rotate and the other leg to ABDuct/externally rotate, presenting as if the legs were “swept” away together to one side of the chair.
What is the spine doing?
Will present usually with a rotation or scoliosis, depending on the position of the pelvis.
What is the head doing?
The neck will go into lateral flexion and may be accompanied by forward flexion.
|
Tip: Windswept deformities are named for the direction the lower extremities are “swept” towards; so, in the above picture, this would be a LEFT windswept deformity. |
FIXED VS FLEXIBLE ABNORMAL POSTURE
Can they move in and out of the abnormal posture? Or is it fixed?
FLEXIBLE = CORRECT
When a posture is FLEXIBLE, the skeleton still moves and equipment should be chosen with the goal to CORRECT the abnormal posture.
GOAL = Prevention from becoming a fixed posture
FIXED = ACCOMMODATE
When a posture is FIXED, the skeleton does not move out of the posture. The patient needs equipment that will ACCOMMODATE the fixed posture, providing optimal support and pressure redistribution.
GOAL = Prevent further progression
Let's now look at an example of how a flexible and a fixed postural abnormality is treated.
Pelvic Obliquity
If Flexible: Correct the abnormal posture by building up the lower side to correct the obliquity and even out the pelvis.
If Fixed: Accommodate for the abnormal posture by "filling in" the higher side for more even weight distribution to protect the protruding bony prominence on the lower side.
*Flexible is also termed reducible; fixed is also termed non-reducible.
Now that you have an understanding of the common abnormal postures, you can easily assess your client’s posture and address what needs to be corrected or accommodated in the wheelchair and seating system.
Resources: Cole, Elizabeth, MSPT, ATP. “Steps in the Provision of Wheeled Mobility and Seating- Part 1.” U.S. Mobility; www.VGM.com.

Lindsey Sharpe, PT, DPT
Clinical Education Manager Rehab Division